Thread
📢Read our new paper:
Analysis suggests Covid-19 boosters likely to cause a net clinical harm to young adults(18-29 yr), where total severe adverse events (SAEs) will outweigh Covid hospitalizations averted
Booster mandates are unethical because:1/13🧵
jme.bmj.com/content/early/2022/12/05/jme-2022-108449
Analysis suggests Covid-19 boosters likely to cause a net clinical harm to young adults(18-29 yr), where total severe adverse events (SAEs) will outweigh Covid hospitalizations averted
Booster mandates are unethical because:1/13🧵
jme.bmj.com/content/early/2022/12/05/jme-2022-108449
In April, Paul Offit stated in a NEJM editorial:"It is now incumbent on CDC to determine who most benefits from booster dosing & educate the public about the limits of mucosal vaccines"
CDC/FDA has NOT conducted risk-benefit analysis for young people 2/13
www.nejm.org/doi/full/10.1056/NEJMe2203329
CDC/FDA has NOT conducted risk-benefit analysis for young people 2/13
www.nejm.org/doi/full/10.1056/NEJMe2203329
So, we took up the challenge.
Over 300 universities & colleges were (as of Sept 2022) mandating boosters across North America (1000 with 2-dose Covid-19 mandates still in place)
Is this a science-based policy?
Is it ethically justified?
3/13
Over 300 universities & colleges were (as of Sept 2022) mandating boosters across North America (1000 with 2-dose Covid-19 mandates still in place)
Is this a science-based policy?
Is it ethically justified?
3/13
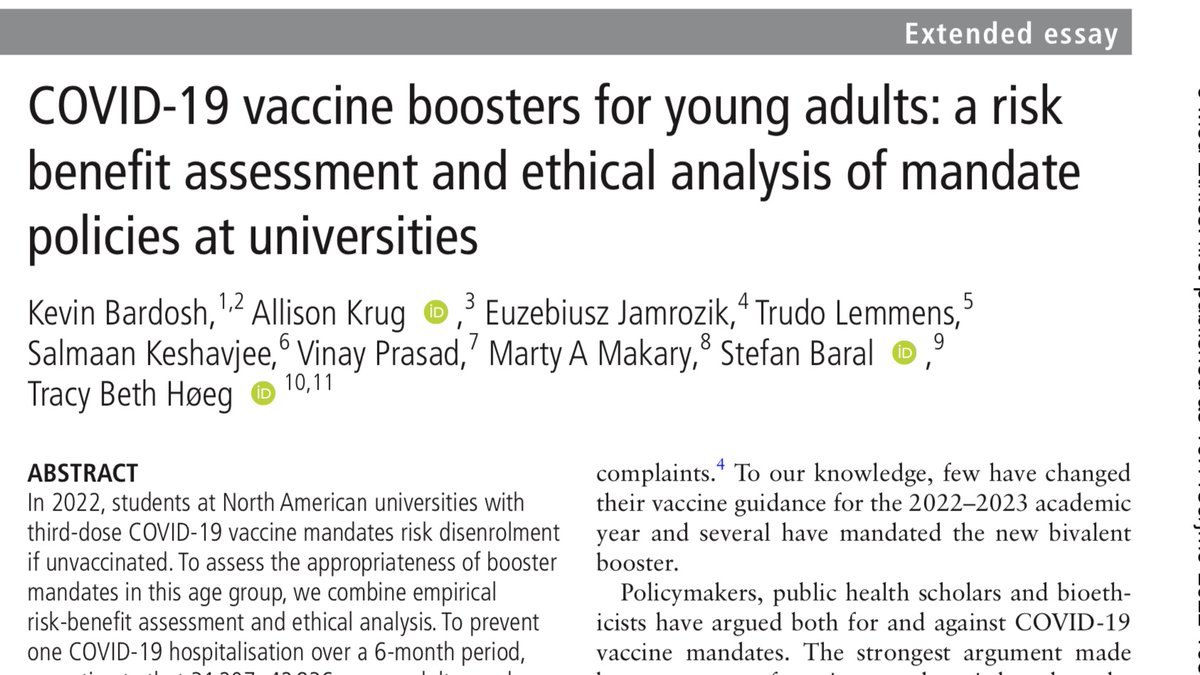
Using CDC/Pfizer data,we estimate 31,207-42,836 previously UNINFECTED adults 18-29 yrs must be boosted to prevent 1 C19 hospitalization over 6 months.But we also estimate 18.5 serious adverse events
Displayed per million boosted:
32 hospitalizations prevented = 593.5 SAEs
4/13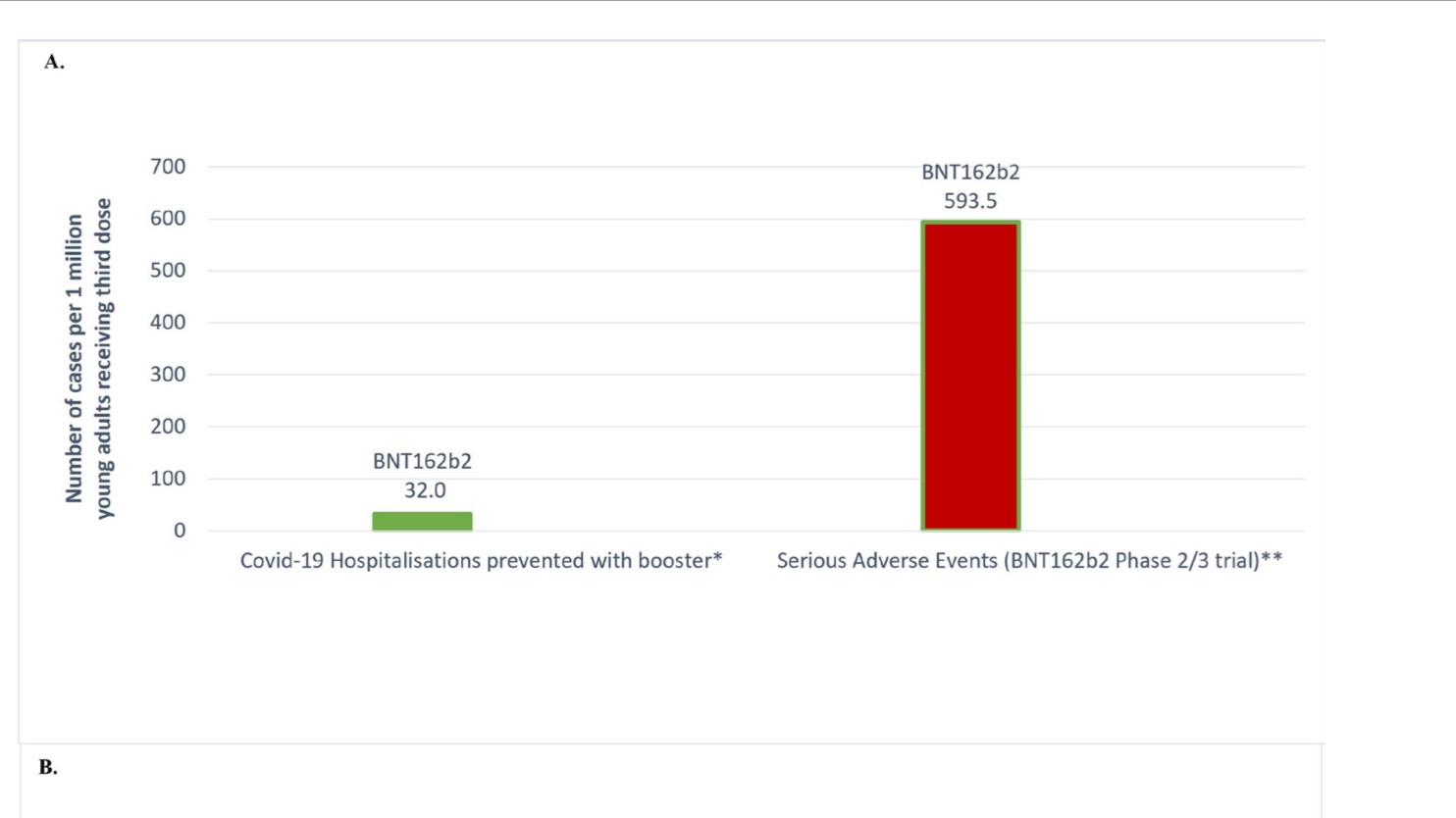
Displayed per million boosted:
32 hospitalizations prevented = 593.5 SAEs
4/13

We also anticipate 1,430–4,626 cases of grade ≥3 reactogenicity per C19 hospitalization averted, which prevents people from conducting daily activities.
Displayed per million boosted, here👇 5/13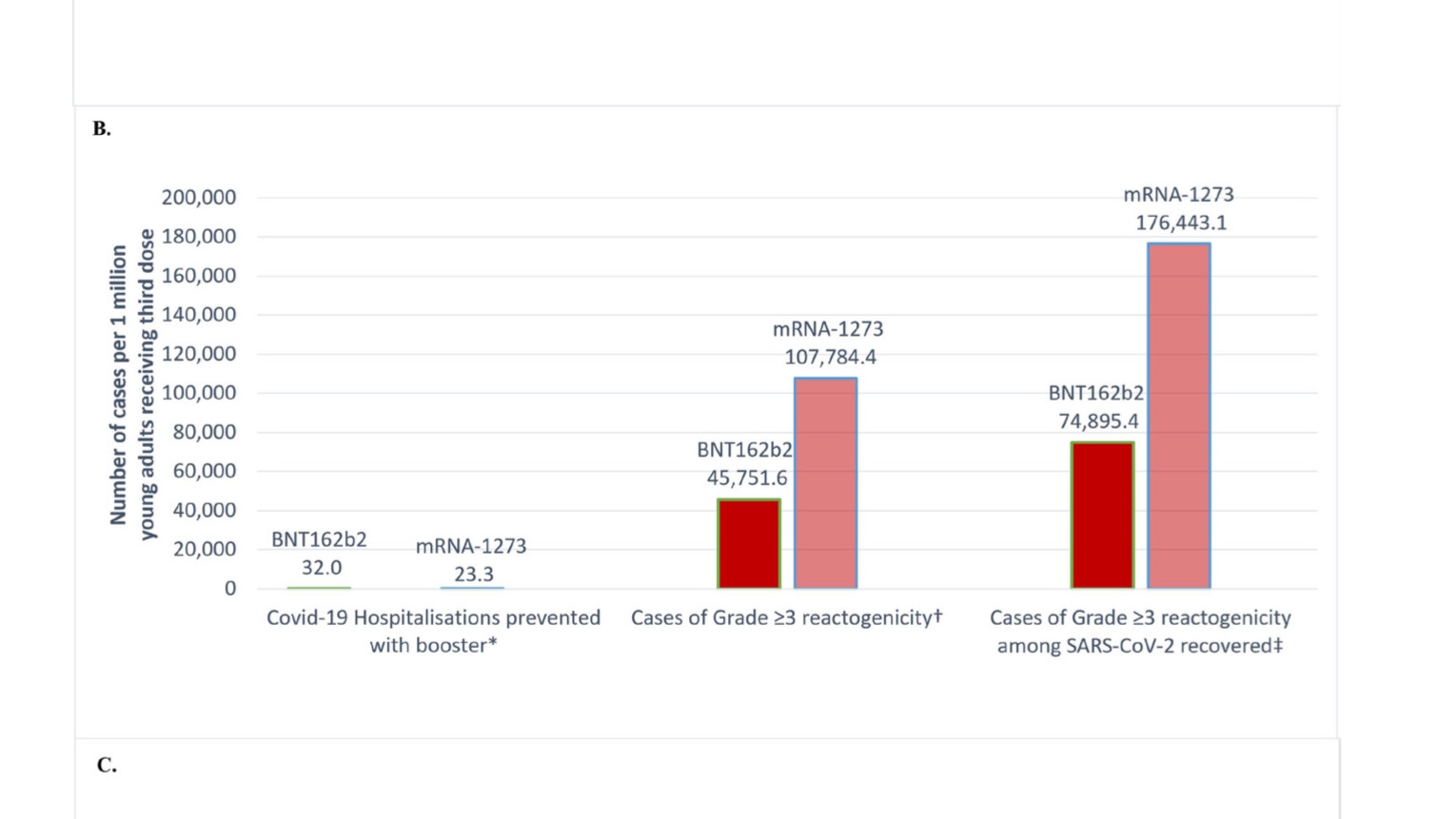
Displayed per million boosted, here👇 5/13

We anticipate 1.5 to 4.6 booster-associated myopericarditis cases in males (typically requiring hospitalisation) per Covid hospitalization averted.
Displayed per million young adults (18-29) boosted here: 👇
6/13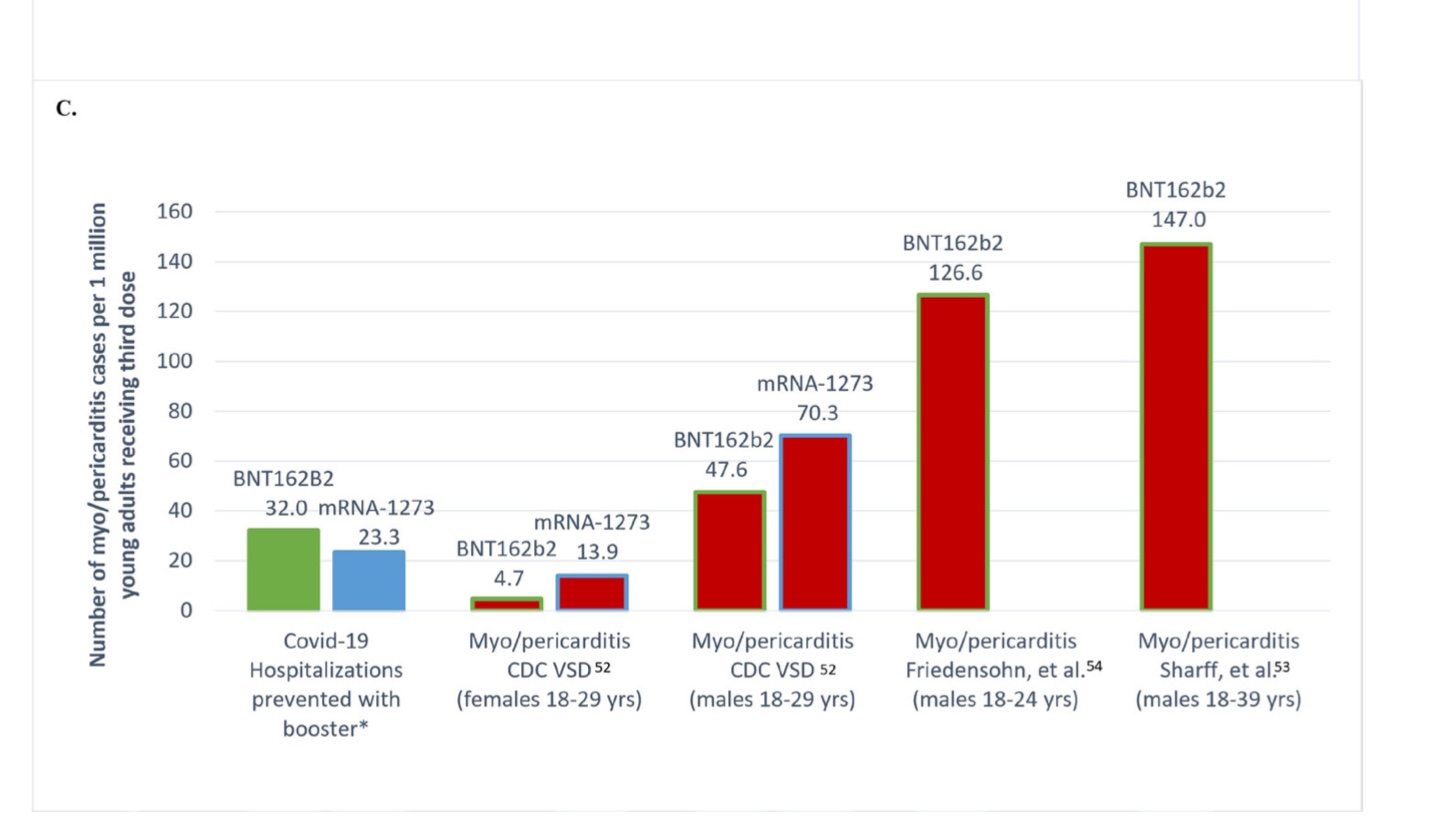
Displayed per million young adults (18-29) boosted here: 👇
6/13

We then outline 5 ethical arguments against booster mandates at institutions of higher education in North America.
1) The CDC has been negligent and it is incumbent on the agency to conduct an updated Omicron risk-benefit analysis for this age group. 7/13
1) The CDC has been negligent and it is incumbent on the agency to conduct an updated Omicron risk-benefit analysis for this age group. 7/13
2) Our analysis (see above) shows the alarming possibility that mandates may result in a net expected harm to young people. This violates the 'do no harm principle.' 8/13
Our estimates assume NO ONE has been infected w Covid. So: real-world benefits likely to be less favourable.
Our estimates assume NO ONE has been infected w Covid. So: real-world benefits likely to be less favourable.
3) Vaccine mandates are not proportionate public policy.
The benefits are unlikely to outweigh the harms by any significant degree to justify liberty restrictions.
Current vaccines do not durably stop transmission.
9/13
The benefits are unlikely to outweigh the harms by any significant degree to justify liberty restrictions.
Current vaccines do not durably stop transmission.
9/13
4) Booster mandates violate the reciprocity principle.
US vaccine injury schemes are completely inadequate and have failed to provide support for rare but severe Covid-19 vaccine injuries. 10/13
US vaccine injury schemes are completely inadequate and have failed to provide support for rare but severe Covid-19 vaccine injuries. 10/13
5) Booster mandates have wider social harms.
Students and faculty risk being dis-enrolled or fired.
Mandates have caused backlash, resistance & anger.
This has further damaged the trustworthiness & credibility of scientific institutions/universities. 11/13
Students and faculty risk being dis-enrolled or fired.
Mandates have caused backlash, resistance & anger.
This has further damaged the trustworthiness & credibility of scientific institutions/universities. 11/13
We consider counter-arguments against our position, such as a desire to 'socialize' compliance & increase safety on campus
We find these arguments sorely lacking in a scientific or ethical basis.
European countries have more appropriate policies for boosters in young pls
12/13
We find these arguments sorely lacking in a scientific or ethical basis.
European countries have more appropriate policies for boosters in young pls
12/13
Lastly, we make the point that although our risk-benefit analysis is focused on boosters in young adults, our analysis is relevant to other university, workplace & school Covid-19 vaccine mandates, esp given high prior infection rate among the US population.
End (@VPrasadMDMPH)
End (@VPrasadMDMPH)
Mentions
See All
Nicholas A. Christakis @NicholasAChristakis
·
Dec 6, 2022
A fine thread and new paper with a detailed clinical and ethical risk-benefit analysis of use of COVID19 boosters in young adults (age 18-29). The evidence would indicate mandating boosters in this age group at present (given current strains & vaccines) is ill advised on balance.