Thread
Last week, child & adolescent physician Dr. McNamara pledged in front of Florida’s Medical Board to provide a “truthful account" of pediatric gender medicine. She then falsely claimed that a key evidence report the Board relied on was invalid, as it was written by a "dentist.” /1
Dr. McNamara failed to mention that the author of the FL analysis (who does have a DDS) holds a PhD in Clinical Epidemiology & Health Care Research & published 140+ peer-reviewed publications on evidence evaluation & clinical practice guideline methods./2
Not only did the FL evidence analysis author train with the "father" of evidence-based medicine, but she now teaches and advances research methods at McMaster's leading center in systematic reviews & clinical practice guidelines development. The Board noted this. /3
When misrepresenting the authors' credentials didn’t work to discredit the FL analysis, McNamara changed tactics. She asserted that the reason the analysis was invalid because it was done by a Canadian team who “violated” the U.S. standards. This, too, is demonstrably false. /4
The "violated standards" McNamara is referring to are in the table below, from a 2011 Institute of Medicine document. These recommended standards are for “systematic reviews of evidence”—not for the "OVERVIEW of systematic reviews" commissioned by FL. /5
nap.nationalacademies.org/catalog/13059/finding-what-works-in-health-care-standards-for-systematic-re...
nap.nationalacademies.org/catalog/13059/finding-what-works-in-health-care-standards-for-systematic-re...

An "overview of systematic reviews,” aka an “umbrella review,” assesses the systematic reviews (SR) themselves, rather than assessing individual studies. By synthesizing findings from multiple SRs, "overviews" mitigate the risk of relying on a single and possibly misleading SR./6
While “systematic reviews of evidence” are still the gold standard for evidence evaluation (as we explained in a recent thread), FL commissioned a different analysis: an evaluation and synthesis of the 𝙖𝙡𝙧𝙚𝙖𝙙𝙮 𝙚𝙭𝙞𝙨𝙩𝙞𝙣𝙜 systematic reviews. /7
The purportedly violated "standards" don't apply to the type of review FL commissioned because it was not a "systematic review of evidence." Further, the author of the analysis is a methodologist with significant "pertinent clinical content area expertise" which she disclosed./8 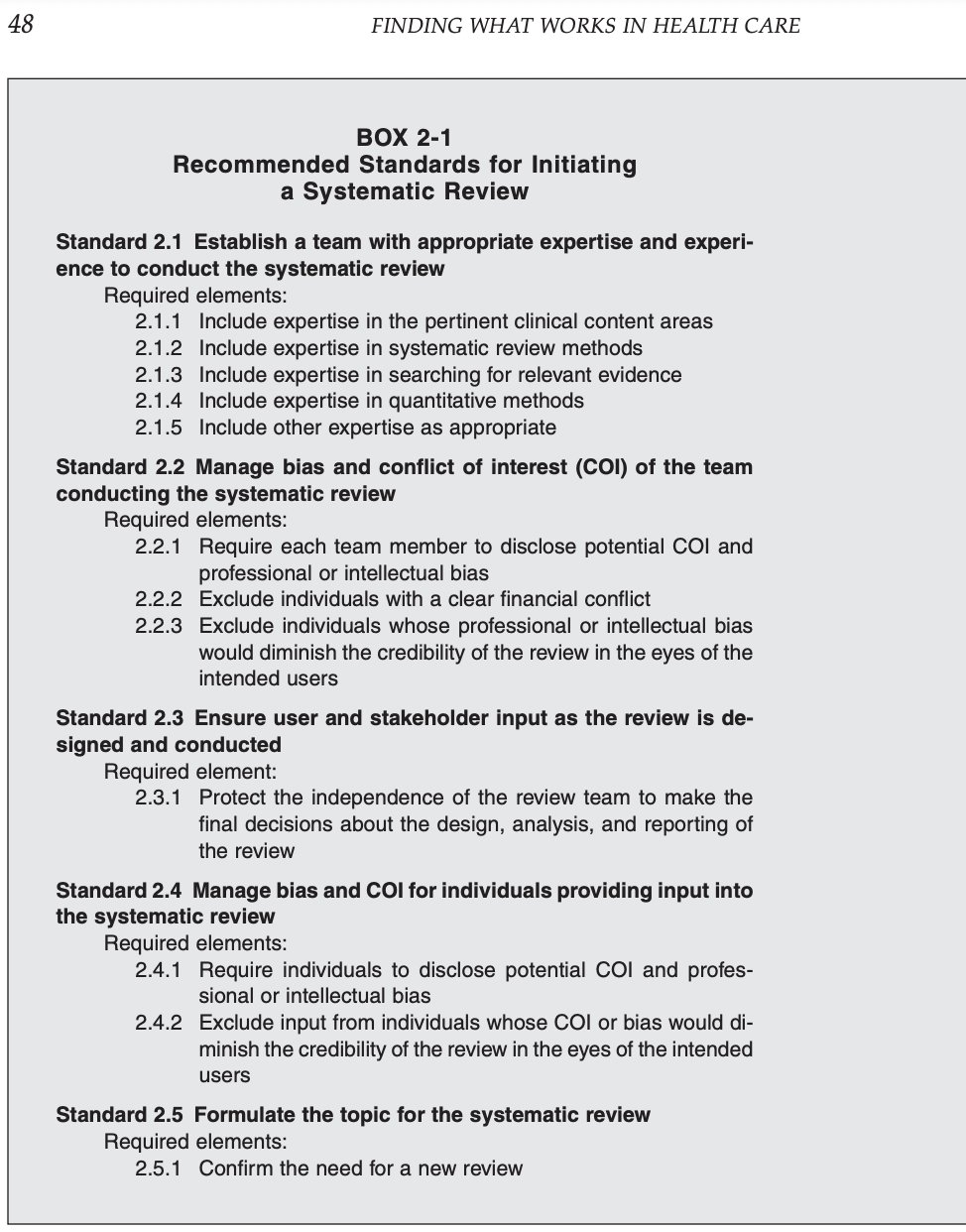

Public health authorities often commission methodologists, not practicing clinicians, to perform evidence evaluation & even lead guideline development. Not having a vested interest is the field allows methodologists to remain impartial, minimizing bias./9
journals.sagepub.com/doi/10.1177/01410768221095240
journals.sagepub.com/doi/10.1177/01410768221095240
The NHS England asked NICE, not WPATH, to review the evidence for a reason. Both individual "field experts" and specialty medical societies can introduce bias into evidence evaluation, ranging from unduly firmly-held intellectual positions, to financial conflicts of interest./10
Like all research, the FL evidence analysis has limitations. What matters is if they are significant enough to alter the conclusions. The FL analysis conclusion of low quality of evidence (for both benefits & risks) mirrors the conclusions of every systematic review to date./11 

McNamara agreed with the report’s “low quality evidence" grading, but insisted that the term “low quality” is inappropriately used to scare "nonexperts." She used the example of low quality evidence leading to a "strong" recommendation to eat fruit to combat childhood obesity./12
To explain why the fruit analogy is not an apt one, we first must explain the GRADE definitions of “very low/low evidence,” which are not hard to grasp. These "grades" signal that the results from the studies that comprise the evidence may not be valid./13
bestpractice.bmj.com/info/us/toolkit/learn-ebm/what-is-grade/
bestpractice.bmj.com/info/us/toolkit/learn-ebm/what-is-grade/
McNamara is right that “low quality" evidence CAN result in a “strong” treatment recommendation. This can happen when the treatment is low-risk (such as eating fruits &veggies). However, puberty blockers & cross-sex hormones have a different risk profile than apples & carrots./14
Low quality evidence can also result in a strong "recommendation AGAINST" when the treatment is associated with severe risks. McNamara's example of a strong recommendation NOT to use aspirin for kids, based on low quality evidence, illustrates this type of situation well. /15
McNamara's discussion on rating the strength of 𝙚𝙫𝙞𝙙𝙚𝙣𝙘𝙚 vs the strength of 𝙧𝙚𝙘𝙤𝙢𝙢𝙚𝙣𝙙𝙖𝙩𝙞𝙤𝙣𝙨 however is moot.𝘽𝙤𝙩𝙝 the quality of evidence AND and the strength of recommendations for puberty blockers & cross sex hormones are rated as “𝙡𝙤𝙬/𝙬𝙚𝙖𝙠.”/16
Other claims made by McNamara during her testimony were also questionable. As an expert in caring for gender-dysphoric youth, she asserted that mastectomies are as rare as "bottom surgery" & assured the Board she’s NEVER met a single patient <25 who wanted—or—got a mastectomy./17
This assertion was met with skepticism from the Board. It also contradicts reports of the rapidly rising rates of hospital-based mastectomies in minors 12yrs+. These numbers are an undercount, since plastic surgeons often use their own surgical centers./18 jamanetwork.com/journals/jamapediatrics/fullarticle/2797439
A recent analysis raised questions whether McNamara sees many gender dysphoric youth given her assertions of never having seen a single minor wanting a mastectomy. Her overall expertise in the field of pediatric gender medicine is also in question./19
www.city-journal.org/floridas-reason-and-compassion-on-gender-medicine
www.city-journal.org/floridas-reason-and-compassion-on-gender-medicine
McNamara and colleagues’ written submission to the FL Board recycled a legal submission in another state. In it, the esteemed “Yale” team accused SEGM of using an “undefined term” “GIDs” (which they had to google), along with displaying an “unverifiable graph” from "GIDS."/20 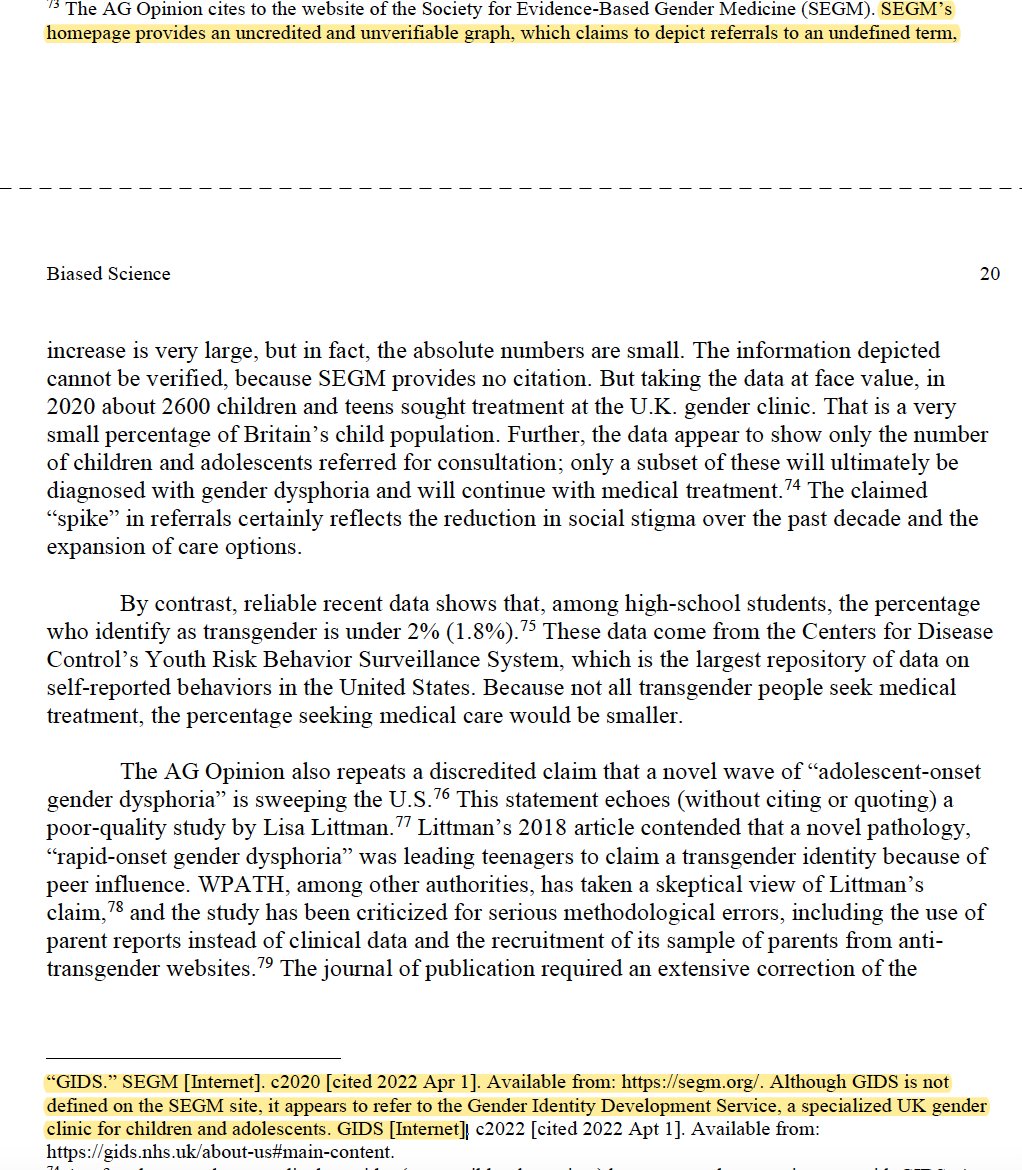

"GIDS" is the largest pediatric gender clinic in the world in the UK. Its graph was the first to demonstrate the recent sharp rise of gender dysphoria in youth (esp. teen females). GIDS is set to shut down in 2023 in large part due to failures of the "affirmative care model."/ 21 

McNamara's lack of familiarity with the term "GIDS" puts into context the credibility of her assertion that the recent European changes in youth gender transitions are "minimal." For those interested, the summary of England's changes can found below./22
segm.org/England-ends-gender-affirming-care
segm.org/England-ends-gender-affirming-care
McNamara’s testimony pleased the crowd but did not impress the Medical Board. Her inability to articulate how one conducts differential diagnosis or determines medical necessity of surgery (beyond a teen's wish), revealed the "Wild West" state of US pediatric gender medicine./23
McNamara’s inability to explain or defend pediatric gender transition can be excused by her lack of experience. What's unclear is why the Endocrine Society, the AAP, and WPATH—the three pillars of pediatric gender affirmation worldwide—failed to show up to defend their work. /24
Dr. McNamara is entitled to her opinion on the Florida Boards' of Medicine decision to curb gender transition of minors. What she is not entitled to is her own version of facts. Sadly, misrepresenting facts has become a go-to tactic for many in the field of gender medicine./25