Thread
1- We can treat depression in older adults.
Psychotherapy is effective in mild-moderate depression, antidepressants in moderate-severe depression.
But what if these don't work? The results of the OPTIMUM study may help.
#GeriTwitter #PsychTwitter
www.nejm.org/doi/full/10.1056/NEJMoa2204462
Psychotherapy is effective in mild-moderate depression, antidepressants in moderate-severe depression.
But what if these don't work? The results of the OPTIMUM study may help.
#GeriTwitter #PsychTwitter
www.nejm.org/doi/full/10.1056/NEJMoa2204462
2- Note: this study focused on pharmacological treatment of late-life depression.
It did not address evidence-based psychotherapies such as cognitive-behavioral therapy & interpersonal therapy or what to do when these don't work.
It did not address evidence-based psychotherapies such as cognitive-behavioral therapy & interpersonal therapy or what to do when these don't work.
3- One of the dilemmas in treating late-life depression with medications is determining whether to switch to another antidepressant or augment w/ a second medication.
Usually we try to keep med regimens as simple as possible b/o risk of side effects and drug-drug interactions.
Usually we try to keep med regimens as simple as possible b/o risk of side effects and drug-drug interactions.
4- The OPTIMUM study attempted to answer the switch vs augment question by randomizing people to:
Step 1: augment w/ aripiprazole OR augment w/ bupropion OR add bupropion
Step 2: augment w/ lithium OR switch to nortriptyline
Step 1: augment w/ aripiprazole OR augment w/ bupropion OR add bupropion
Step 2: augment w/ lithium OR switch to nortriptyline

5- The study recruited people 60 years and older whose current episode of major depression had not remitted after two antidepressant trials.
They had to be on an antidepressant already at the start of the trial.
A total of 619 people were enrolled. See Table 1 for demographics.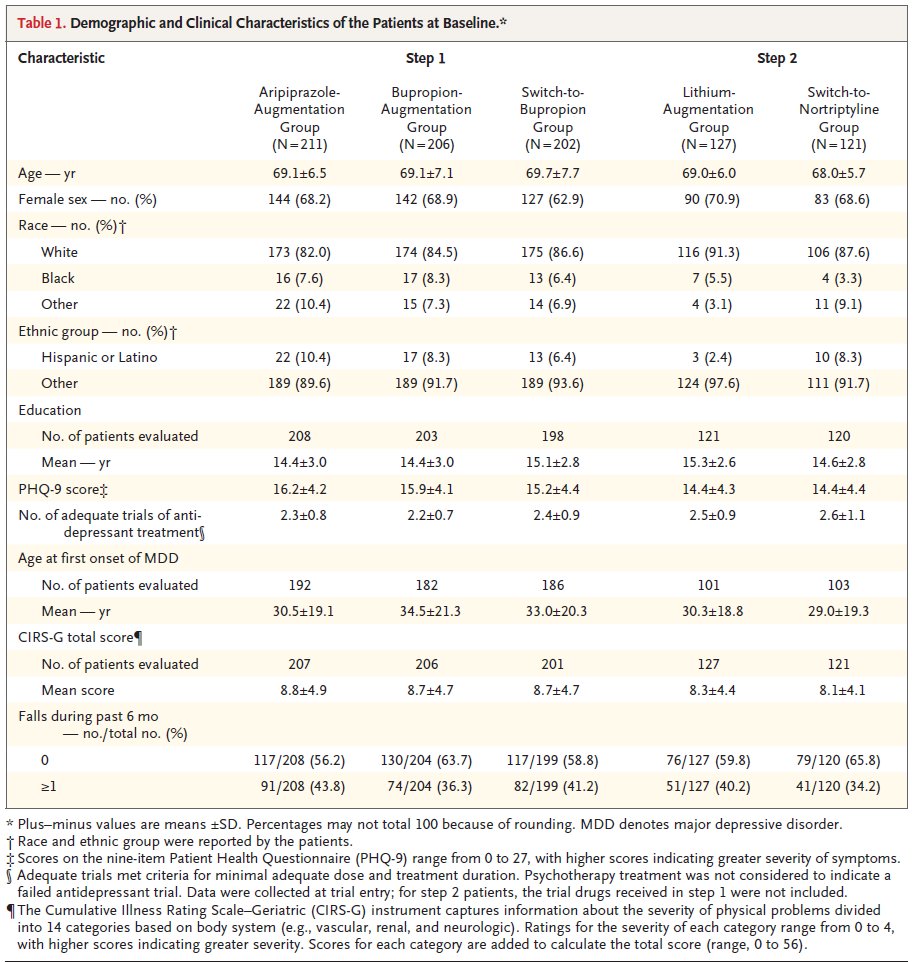
They had to be on an antidepressant already at the start of the trial.
A total of 619 people were enrolled. See Table 1 for demographics.

6- What were the results?
Remission rates (MADRS<10) after 10 weeks ranged from 18.9% to 28.9%. These seem low, but they are consistent w/ treatment-resistant depression.
Augmenting w/ aripiprazole (28.9%) or w/ bupropion (28.2%) was most effective.
Remission rates (MADRS<10) after 10 weeks ranged from 18.9% to 28.9%. These seem low, but they are consistent w/ treatment-resistant depression.
Augmenting w/ aripiprazole (28.9%) or w/ bupropion (28.2%) was most effective.

7a- The primary outcome was psychological wellbeing, measured by the NIH Toolbox Emotion Battery subscales for Positive Affect & General Life Satisfaction.
Authors note that this was "chosen to reflect the stakeholder-driven trial design," i.e., patients asked for this outcome.
Authors note that this was "chosen to reflect the stakeholder-driven trial design," i.e., patients asked for this outcome.
7b- On the measure of psychological wellbeing, the only statistically significant difference was that augmenting with aripiprazole was more effective than switching to bupropion.
9- How about safety, a critical issue in treating older adults?
Falls are particularly concerning - and were the most common side effect in this study.
Interestingly, adding bupropion had the worst outcomes w/r/t falls. I've listed the other most common side effects below.
Falls are particularly concerning - and were the most common side effect in this study.
Interestingly, adding bupropion had the worst outcomes w/r/t falls. I've listed the other most common side effects below.

10- Caveats:
- Study was not blinded, i.e., patients knew which treatment they got.
- Only 40-70% of patients adhered to the regimen.
- Treatment of 10 wks may be too brief.
- They did not recruit as many patients from underrepresented racial/ethnic minorities as planned.
- Study was not blinded, i.e., patients knew which treatment they got.
- Only 40-70% of patients adhered to the regimen.
- Treatment of 10 wks may be too brief.
- They did not recruit as many patients from underrepresented racial/ethnic minorities as planned.
11- Funding source: The Patient-Centered Outcomes Research Institute (PCORI).
PCORI is an independent, non-profit organization and is the leading funder of comparative effectiveness research in the US.
PCORI is an independent, non-profit organization and is the leading funder of comparative effectiveness research in the US.
12a- Summary:
While these results are not dramatic, treatment-resistant depression is frustrating for patients & their families.
Since the preliminary results came out last year, I have been less dogmatic about switching in order to avoid polypharmacy & more open to augmenting.
While these results are not dramatic, treatment-resistant depression is frustrating for patients & their families.
Since the preliminary results came out last year, I have been less dogmatic about switching in order to avoid polypharmacy & more open to augmenting.
12b - Of course, I would still be cautious using these medications, especially in combination. The risk of falls is high & worrisome.
And we need to make sure that older adults w/ depression have access to psychotherapy, exercise & activities that support meaning & purpose. /end
And we need to make sure that older adults w/ depression have access to psychotherapy, exercise & activities that support meaning & purpose. /end
Mentions
See All
Awais Aftab @awaisaftab
·
Apr 2, 2023
Very helpful thread, thank you.